What Does PCA Mean in Medical Billing?
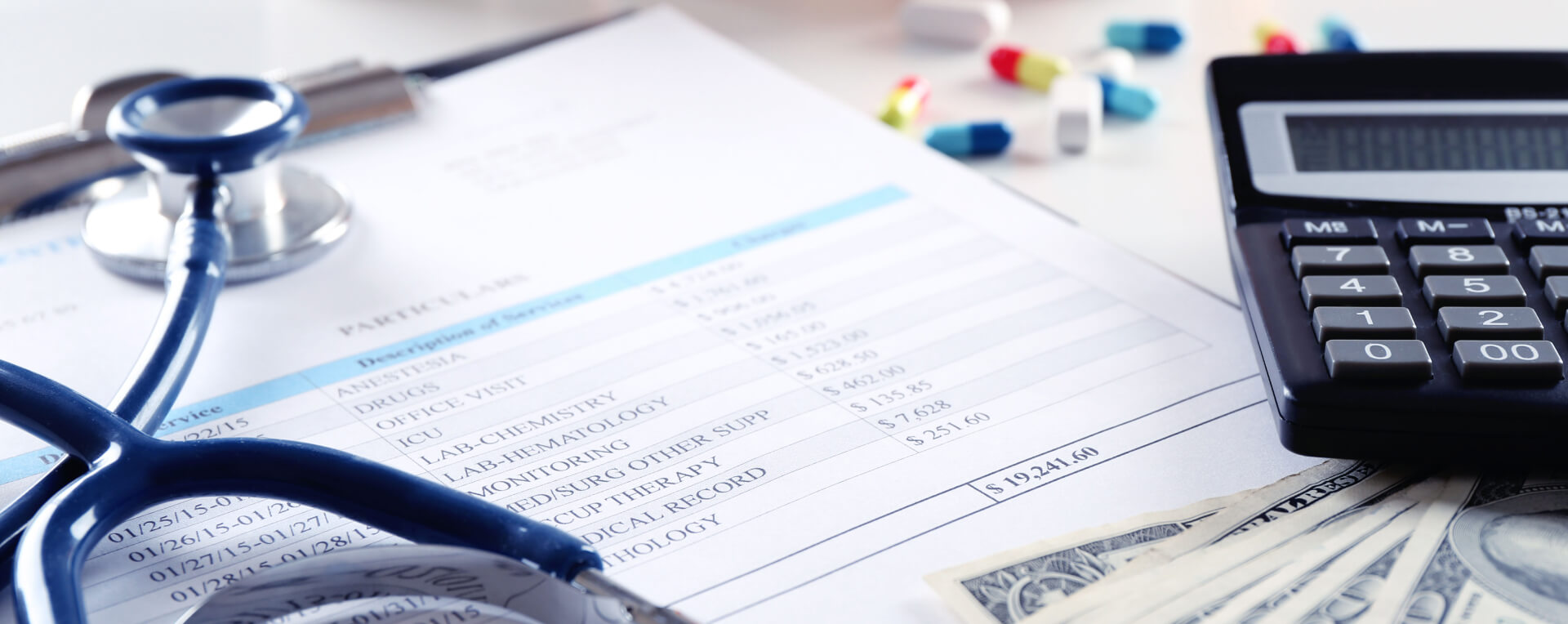
Claim errors are still a major problem for healthcare practices. In Experian Health’s 2025 State of Claims findings, 41% of providers said at least 10% of their claims were denied, and 68% said inaccurate or incomplete patient data at intake drives denials. That matters because even a small misunderstanding in documentation or coding can slow payment and create rework. This blog explains what patient-controlled analgesia (PCA) means, where the term shows up in billing, and what teams should check before a claim goes out.
In most hospital and pain-management billing discussions, PCA usually means patient-controlled analgesia. The National Cancer Institute defines it as a method of pain relief in which the patient receives a preset dose of medicine by pressing a button on a computerized pump. It is often used after surgery and may also be used for painful conditions such as pancreatitis or sickle cell disease.
Here is the part many people skip. In some Medicaid home-care settings, "PCA" can also mean "personal care attendant." The Centers for Medicare & Medicaid Services (CMS) uses that meaning in its personal care services resources and discusses how improper billing can happen when providers do not follow state Medicaid rules. So, the right meaning depends on the setting. In acute care and anesthesia billing, PCA usually refers to patient-controlled analgesia. In home-based personal care claims, it may refer to the worker providing the service.
What exactly does PCA mean in medical billing?
When people search for PCA in medical billing, they are usually asking about patient-controlled analgesia. This is a pain-control method that lets the patient self-administer a programmed dose of medication through a pump. It may be delivered through an IV line, an epidural catheter, a peripheral nerve catheter, or, in some settings, through other delivery systems. Clinical sources note that PCA is commonly used for acute, chronic, postoperative, and labor pain and that it often improves pain control and patient satisfaction compared with waiting for nurse-administered doses.
For billing teams, the key point is simple. PCA is not just a device term. It affects documentation, charge capture, medical necessity review, route of administration, and whether any part of the service is separately reportable. That is why the abbreviation matters in the revenue cycle, not only in clinical notes.
Why does PCA create billing confusion?
The biggest reason is that PCA is a shared abbreviation. In one setting, it refers to patient-controlled analgesia. In another, the Centers for Medicare & Medicaid Services (CMS) uses it in personal care services to describe a personal care attendant. If a billing team sees “PCA” in a note without enough context, the abbreviation alone does not explain the service.
Confusion also happens when documentation is too short. A chart may say “patient on PCA” without clearly showing the route, the ordering provider, who managed the pain service after surgery, or whether the service was part of routine postoperative care. That is where claim edits and payment delays begin. Clear words beat short notes every time.
How is PCA billed?
This is where accuracy matters most. The Medicare policy shows that postoperative pain management is generally included in the global surgical package when it is handled by the physician performing the surgery. CMS also states that routine management of patient-controlled analgesia is not reimbursable to another physician or provider as a separate anesthesia or E&M service.
There are exceptions, but they are specific. CMS guidance explains that daily hospital management of epidural or subarachnoid continuous drug administration may be reported with the Current Procedural Terminology (CPT) code 01996 on days after catheter placement, not on the day of surgery. CMS also notes that separate reporting may apply when an anesthesia practitioner takes over postoperative pain management under the right circumstances and documentation supports that handoff. Medical billing depends on the route used, the date of service, who managed the pain care, and whether the service was already bundled into the surgical or anesthesia package.
What should billing teams check before filing a PCA claim?
Start with the record. Make sure the note clearly shows whether PCA means patient-controlled analgesia or something else. Then check the route used, such as IV, epidural, or a peripheral nerve catheter. Confirm who placed the catheter, who managed the pain service after surgery, and whether that management was routine or separately requested. Finally, review payer-specific rules before coding because Medicare rules and Medicaid personal care rules do not treat every PCA-related service the same way.
Who should review PCA workflows more closely?
Practices should take a closer look if they see repeated denials tied to postoperative pain management, unclear anesthesia documentation, or confusion between hospital pain services and home-based personal care services. This matters even more for organizations handling surgery, pain management, hospice, or Medicaid-supported home care, because the same abbreviation may carry different billing consequences across those service lines.
What are the most common billing mistakes linked to PCA?
One common mistake is treating all PCA-related care as separately billable. CMS guidance shows that this is not true, especially when the service is part of routine postoperative care or part of the anesthesia service on the same date.
Another mistake is weak wording in the chart. If the documentation only says “PCA started” without describing the route, timing, provider role, or postoperative management arrangement, coders may not have enough support for the claim. A third mistake is assuming the abbreviation means the same thing in every setting, even though CMS uses PCA differently in personal care services materials.
When is outside billing help worth considering?
Outside support may make sense when claims are delayed by bundling edits, modifier issues, unclear documentation handoffs, or repeated staff confusion around anesthesia and postoperative pain rules. A focused billing review can help a practice find where PCA in medical billing is being misunderstood before those errors turn into lost revenue or compliance risk.
Need help reviewing pain-management documentation, bundled services, and anesthesia-related claim issues before they affect payment? If you need any help, connect with Capline's experts; book a consultation call with our billing specialists.
FAQs
Is PCA always patient-controlled analgesia?
No. In many hospital billing discussions, it means patient-controlled analgesia. In some Medicaid personal care programs, it can mean a personal care attendant. The setting decides the meaning.
Is routine PCA management separately billable?
Not usually. CMS states that routine postoperative PCA management is generally part of the surgeon’s postoperative management and is included in the global surgery fee.
Can CPT 01996 be billed for PCA?
It can apply to daily hospital management of epidural or subarachnoid continuous drug administration on days after catheter placement, but not on the day of surgery. It does not apply broadly to every PCA situation.
What is the biggest billing risk with PCA?
The biggest risk is unclear documentation. If the record does not show the meaning of PCA, the route, the provider role, and whether the service was bundled or distinct, the claim is more likely to be denied or paid incorrectly.